




“Those who cannot remember the past are condemned to repeat it.”
George Santayana, The Life of Reason: The Phases of Human Progress
1. Introduction
It should be inevitable that the health professions learn from the experience of treating the epidemic of injuries arising from war, alongside addressing the issues in preventive medicine needed to maintain the medical fitness of the force (DeBakey, 1996: 711-716). The clinical challenges associated with the care of war injured that lead to advances in pre-hospital care, medical evacuation, hospital care, and rehabilitation have implications for civilian practice (Chatfield-Ball, et al., 2015: 93-100). However, not all these advances are incremental. Often old lessons from military medicine must be re-learned by a new generation and it takes time to mobilise the research systems that generate new knowledge (DeBakey, 1947: 341-350). The extent to which this knowledge becomes engrained within the military medical system also varies according to the enduring status of medicine within the military and the memories of clinicians (Walker, 2018: 173-176). This paper will examine the legacies of the Korean War for modern military medicine by considering how the themes described in various contemporary sources have been extrapolated into military medical practice in the 21st Century. The paper will start by setting the Korean War in the context of ‘Western Wars’, and the factors that influenced military medical planning. It will then describe a framework for analysis based on a framework for categorising the functions of a complete military health system using the current military medical concepts of ‘The Operational Patient Care Pathway’ and the ‘10 Instruments of Military Healthcare’ (Bricknell, et al., 2015: 9-14). The instruments are: Medical Command, Control, Communications, Computers (MedC4I); Force Health Protection (FHP); Pre-hospital Emergency Care (PHEC); Medical Evacuation (MEDEVAC/TACEVAC/STRATEVAC); Primary Health Care (PHC); Deployed Hospital Care (DHC); Role 4/Firm Base; Medical Logistics; the Medical Contribution to Security and Stabilisation; and Research and Innovation. Each of these ‘instruments’ will be considered in separate sections of the paper, reflecting on the insights from the Korean War through to contemporary academic papers. It will close by considering the performance of whole military medical system during the Korean War in comparison with later wars and conclude by considering the implications for learning lessons from history.
2. Context
The interpretation of the impact of the Korean War on military medicine needs to be placed within the historical context of this conflict from a ‘Western’ (primarily US) perspective as ‘sandwiched’ between World War II and the Vietnam War. World War II led to significant changes in the organisation of military medical care. Most nations’ health professionals were involved in caring for casualties of that war, both military and civilian. There were substantial advances in clinical topics across preventive medicine, resuscitation, surgery, infectious disease, and rehabilitation. These have been covered by medical ‘official histories’ of the Second World War published by the governments of the United States1) and Commonwealth Countries (MacNalty and Mellor, 1968), many other books, and academic papers. The experience from World War II provided the foundations for many of the advances in military medicine that occurred during the Korean War. In turn, many of the lessons from the Korean War acted as foundations for military medical developments during the Vietnam War and subsequently. Unfortunately, there are also examples of military medical innovation being forgotten and being relearned.
The Korean War occurred within a country that had been colonised by Japan from 1910 until the end of the Second World War. After the withdrawal of Japanese forces in 1945, the country was divided along the 38th parallel into a Northern occupation zone controlled by Soviet Russia and a Southern occupation zone controlled by the United States. Responsibility for the military government in the South lay under the Supreme Command for the Allied Powers (SCAP) led by General Douglas McArthur based in Japan. South Korea achieved sovereign independence as the Republic of Korea (ROK) on 15 August 1948. Many institutions in ROK, including the armed forces and the public health system, lacked indigenous capacity. The Allies provided military and civilian support to capacity building programmes in many areas of government including public health and military health. Thus, any analysis of medical lessons from the Korean War needs to consider this dimension as well as advances in military clinical practice within international forces.
The Korean War can be considered as a high intensity ‘state-on-state’ conflict fought between strategic political coalition partners (North Korea and communist supporters Russia and China, against South Korea and supporters under the United Nations Command including the United States (US), United Kingdom (UK), Australia, Belgium, Canada, Colombia, Ethiopia, France, Greece, Luxembourg Netherlands, New Zealand, Philippines, Thailand, Turkey, and South Africa). It was fought using modern conventional weapons (by the standards of the 1950s). The war occurred a long way from these United Nations (UN) countries, in a relatively underdeveloped country with limited strategic infrastructure (roads, railways etc). The environment posed significant health threats including heat, cold, and infectious disease. These factors had significant implications on the military medical system. The war was characterised by an initial highly mobile phase across the entire Korean peninsula during 1950 followed by stalemate along the 38th parallel from 1951-1953. This had implications for the mobilisation and evolution of the ROK and UN military medical support plan until the cessation of hostilities in 1953.
The Korean War lasted 3 years. The US recorded 33,686 combat deaths, ranking the war 5th for US military deaths behind World War II, the American Civil War, World War I and the Vietnam War.2) For the UK, it caused the most intense loss of life in the armed forces since Second World War (1,120 deaths), compared to 1,442 deaths in Malaya over 12 years, 1,441 deaths in Northern Ireland over 38 years and 467 deaths in Afghanistan over 11 years.3) These figures pale into insignificance when considering the impact on the Korean population, with an estimated 2,240,000 deaths from Korean War as the largest cause of deaths from conflict since 1945 (Khorram-Manesh, et al., 2021: 1-11). If one assumes a ratio of 3 injured for every battle death (Khorram-Manesh, et al., 2022: e313-e321), the substantial numbers of battle casualties will have been a stimulus for advances in military medicine but the short duration of the war may have hindered the full exploitation of this experience. Thus, any assessment of the contribution of the Korean War to the subsequent progress of military medicine needs to be considered in the context of the wars that followed, most specifically the Vietnam War and the 21st Century conflicts in Iraq and Afghanistan.
3. Analytical Approach
The organisation of a military medical system is often codified within military publications collectively termed ‘military medical doctrine’. Current military medical doctrine summarises overall capabilities of a military health system as a ‘patient care pathway’ from prevention through to rehabilitation and recovery (Bricknell, 2014: 64-69). This concept defines the clinical activities that need to occur at each stage in the care of the military patient, and the organisation of medical treatment and evacuation facilities needed to deliver this care. British military medical doctrine describes the individual elements of a military health system as the 10 Instruments of Military Healthcare: Medical Command, Control, Communications, Computers (MedC4I); Force Health Protection (FHP); Pre-hospital Emergency Care (PHEC); Medical Evacuation (MEDEVAC/TACEVAC/STRATEVAC); Primary Health Care (PHC); Deployed Hospital Care (DHC); Role 4/Firm Base; Medical Logistics; the Medical Contribution to Security and Stabilisation; and Research and Innovation. This categorisation has been used as a structure for this paper.
Most publications on the medical lessons from the Korean War originate from the US armed forces. The primary sources for this paper are The Medic’s War by Albert Cowdrey (Cowdrey, 1987) and the papers from the US conference course titled Recent Advances in Medicine and Surgery held at the US Army Medical Services Graduate School in 1954.4) Other published US sources include the Medical Bulletin of the US Army in the Far East, and Military Surgeon (the forerunner to the current US journal, Military Medicine). The Journal of the Royal Army Medical Corps provides the most sources for the UK contemporary experience, especially the paper by Anderton, the UK divisional surgeon (Anderton, 1953: 43-54). The contemporary evidence from these records have then been interpreted in the light of identified medical lessons from subsequent wars, primarily Vietnam (Neel, 1991), Iraq and Afghanistan (Greaves, 2018; Kellermann, et al., 2017), and also the UK campaign in Northern Ireland (Owen-Smith, 1981: 31-54), and the Falklands War (Batty, 1999: 336-340). This review does not use unpublished primary documents held in individual historical archives.
4. Medical Command, Control, Communications, Computers, and Information (MedC4I)
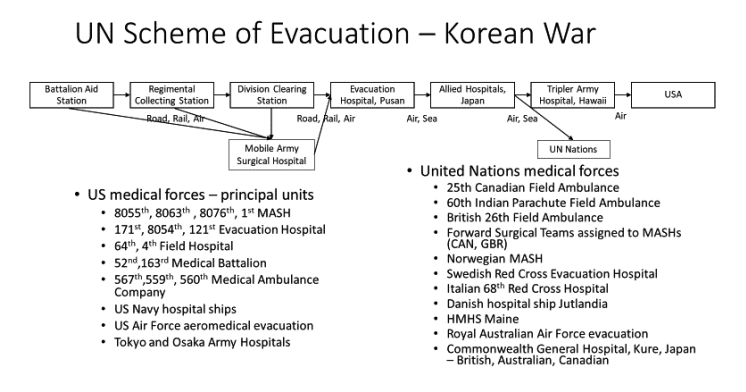
MedC4I covers the design of the patient care pathway and its management through medical leadership (command and control), the method of communications (communications and computers) and the management of information for decision-making. By 1950, the World War II Allies’ military medical services were undergoing demobilisation and reduction in military medical capacity afforded by the outbreak of peace in 1945. This resulted in military medical systems that had to be rapidly expanded for a new war including the mobilisation of junior doctors without previous military experience. Fortunately, the senior military medical leadership had extensive war experience. The long chain of evacuation back to the parent nation for UN international forces mirrored the arrangements for campaigns in Asia against the Japanese during World War II whereby casualties were evacuated from the combat zone and then consolidated in large evacuation hospitals prior to transfer by hospital ship back to their home country. The SCAF hospitals established in Kure, Japan to care for the Allied occupation forces in the region provided the strategic distribution point to which international UN casualties were evacuated from Korea and then dispersed to their parent country. The basic UN scheme of evacuation is shown in Figure 1. After first aid in the field, initial care was provided at the Battalion Aid Station, and clearing of casualties from the battlefield was undertaken by Brigade (Regimental) and Divisional medical units. The first level of surgery was undertaken in the Mobile Army Surgical Hospital (MASH). This was a new US Army unit developed in the late 1940s to consolidate the lessons on mobile surgical units from the Second World War. Casualties were moved by road, train, and air to evacuation hospitals in Busan at the Southern tip of Korea prior to transfer to consolidating them in military hospitals in Japan (US hospitals and the Commonwealth General Hospital, Kure). Movement from the Asia-Pacific region to base hospitals in the US or other United Nations’ home countries was initially done using hospital ships. Later, patients were transferred using strategic aeromedical evacuation aircraft. Whilst the US underwrote the military medical system, it was a true UN effort with the British Commonwealth Division being supported by the 25th Canadian Field Ambulance, the 60th Indian Parachute Field Ambulance5) and the British 26th Field Ambulance (Binning, 1953: 349). The UN medical services provided surgical care in Korea for all combat injured (US, British, Turkish, Filipino, Greek, Thai, Dutch, and Korean military, civilian and prisoners). As well as placing Allied field surgical teams within the US MASHs, the whole medical system was later augmented by the Norwegian MASH (NORMASH) (Lockertsen, et al., 2019: 93-126), the Swedish Red Cross Evacuation Hospital (Östberg, 2014: 133-156), the Italian 68th Red Cross hospital (Kim and Yang, 2022: 127-147), and the Danish hospital ship Jutlandia (Winge, 1996: 102-130).
The Royal Australian Air Force supported the aeromedical evacuation service operated by the US Air Force and HMHS (His Majesty’s Hospital Ship) Maine (Bennett, 1951: 72-86) from the British Royal Navy supported the US Navy in the movement of casualties by sea from Korea to Japan. Whilst the US provided the backbone to the scheme of evacuation, this was a multinational medical force that also included ROK medical units to care for ROK casualties. The importance of this will be considered further under the topic ‘medical contribution to security and stabilisation’. Overall, the UN medical services provided mutual support across each nation’s medical contributions and cared for military casualties of all nations, prisoners of war, and civilians.
The UN scheme of evacuation, shown in Figure 1, reflects the overall design of a military ‘care pathway’ that remains unchanged to the present day. Although the intensity of combat and local conditions will affect the tactical approach to medical evacuation in the forward combat zones, the primary challenge of balancing medical care with medical evacuation whilst moving patients from overseas theatres to their home nation persists. The overall design used during the Korean War applied to the ‘care pathway’ during the Vietnam War, including the use of the Tripler Army Hospital in Hawaii as the strategic intermediate evacuation hospital for US patients from the Asia-Pacific region prior to aeromedical evacuation to the continental USA. The same principles have also applied for the conflicts in the US Central Command area of operations (Iraq and Afghanistan) with patients being aggregated into a primary military hospital in each country (Balad in Iraq, and Bagram in Afghanistan) with the US Army hospital at Landstuhl, Germany filling the same role as the Tripler Army Hospital by acting as an intermediate hospital in the movement of US casualties between continents. Medical support arrangements for coalition forces in both Iraq and Afghanistan also followed similar arrangements with each country contributing medical forces as a proportion of their overall troop strength. Medical units from each country provided mutual support during these wars with US leading and underwriting the overall system (Bricknell, 2007: 44-51). This shows that the overall military medical system needs to operate as a ‘care pathway’ within the capacity and capability of individual elements tailored to the demands of a particular military campaign.
5. Force Health Protection (FHP)
FHP covers all the measures necessary to promote health and prevent disease amongst the military force. South Korea presented a challenging environment in which to fight a war. The main area of operations is mountainous and experiences extremes of hot weather in the summer, and especially cold weather in the winter. The bad winter of 1950/51 resulted in large numbers of soldiers succumbing to cold injuries, hypothermia, and frostbite. Consequently, special protective clothing and equipment was issued alongside a programme of training in the prevention of cold injury. It is notable that, 30 years later, non-freezing cold injury had a significant impact on UK forces during the Falklands War, partially due to inadequate military boots (Craig, 1984: 89). Heat injury was a particular challenge during the first phase of operations in Iraq in 2003 resulting in active prevention policies that were applied for subsequent phases of the campaign (Bolton, et al., 2006: 148-155).
By the end of 19th Century, infectious disease rather than battle injury was the primary cause of death in armies. This scourge was overcome during the first half of the 20th Century through better understanding of the causes of disease, improved diagnostic techniques, the advent of vaccination, and the introduction of penicillin and other antibiotics. The list of diseases endemic to Korea is very familiar to military doctors: smallpox, cholera, typhus, filariasis, Japanese encephalitis, malaria, dysentery, venereal disease (VD). The application of routine preventive measures ensured that diseases did not have a significant impact on UN military operations. These measures included extending vaccination programmes to Korean military recruits, both to protect them and to reduce the risk of transmission of disease to their international allies (Yoon, 1953: 190-191). The prevention of these diseases was much a more significant problem in the Korean civilian community, especially amongst internally displaced populations. Military assistance to civilians was done as much to protect the military forces as for humanitarian purposes. It reinforces the need for military public health experts to monitor the health of the whole population in a theatre of military operations. Finally, within the topic of infectious diseases, there was a strategic concern about the potential use of biological weapons that resulted in a secret mission to evaluate reports of an outbreak of bubonic plague amongst North Korean soldiers (Zimmerman, 2009: 80-83). Whilst not core to this analysis, it is a timely reminder of the potential use of infective agents as a weapon of war.
Body armour was introduced as a universal issue for the first time during the Korean War. This was based on evidence collected by a formal research programme that conducted post-mortem examinations on military casualties to determine the wounding agent (bullet or shrapnel), location, and cause of death (Holmes, et al., 1954: 1477-1478). This led to the design of the ‘flak jacket’ that provided protection against low velocity fragmentation wounds. These were issued after a series of field trials to establish their effectiveness and acceptance for use. This experience led to the establishment of military post-mortem research programmes in Vietnam (Wound Data and Munitions Effectiveness Team), North Ireland (Hostile Action Casualty System) (Mellor and Cooper, 1989: 1006-1010) and Iraq/Afghanistan (Breeze, et al., 2015: 36-41; Eastridge, et al., 2012: S431-S437) to inform the further development of protective body armour; which is in almost ubiquitous use by 21st century armed forces.
6. Pre-hospital Emergency Care and Primary Healthcare
Most deaths on the battlefield occur prior to arriving at hospital. This necessitates a system of pre-hospital emergency care combined with the primary healthcare services that treat disease and non-battle injury. The military units with this role are the Battalion Aid Station and Regimental Collection Station shown in Figure 1. The major causes of preventable death on the battlefield are bleeding, compromised breathing, and wound shock. Pre-hospital care depends on good first aid, stabilisation (including antibiotics and pain relief), and rapid transport to a surgical facility. Scott’s paper on the care of the battle casualty in advance of the Aid Station covers many of the same points that would be taught to a doctor joining the armed forces today, especially his emphasis on resuscitation as a continuum from first aid to surgery (Scott, 1954: 46-57) - similar to the current concept of ‘damage control resuscitation’ (Hodgetts, et al., 2007: 299-300). The pre-hospital use of the tourniquet has been credited with saving many lives in the 21st Century (Kragh Jr, et al., 2015: 184-190). Whilst this has been well understood across the history of military medicine and was re-emphasised from experience during the Korean War, their use in the military environment is probably an example of a lesson ‘unlearned’ as they had to be re-introduced by Western military medical services in the 2000s (Kragh Jr, et al., 2012: 242-252). The Korean War saw the introduction of intravenous administration of re-constituted dried plasma and plasma expanders (such as Dextran) forward of hospitals to combat hypovolaemic shock (Amspacher and Curreri, 1953: 730-740). The story of the role and utility of non-blood intravenous fluids in the pre-hospital care of the combat casualty is a complete history lesson in the science and politics of innovation in military medicine (Blackbourne, et al., 2012: S372-S377; Hooper, et al., 2014: 90-97). It is notable that Scott describes both the administration of morphine and penicillin using pre-packaged syrettes. Pre-hospital analgesia has matured and alternative formulations are now available to enable administration of powerful analgesics via an autoinjector, the inhaled route, or under the tongue (Rogers, et al., 2018: 458-462). However, the penicillin syrette was discontinued and there is currently no pre-mixed antibiotic for parenteral use in the military environment. It has not been possible to determine if this has been a conscious decision or a lesson forgotten.
Although the treatment of battle casualties is important, most of the work of the pre-hospital team (medics and the doctors at the Battalion Aid Station) concerns primary health care. Assessment of disease and non-battle injury, administration of vaccinations, hygiene inspections, assessment of mental health, and treatment of VD is the routine business. Primary healthcare also covers dentistry, musculoskeletal rehabilitation, and field mental health (which will be considered as a separate topic). It is noticeable that the Commonwealth Division deployed a Canadian Field Dressing Station as a small convalescent hospital to enable the early recovery of the lightly wounded and sick within the divisional area (Hunter and Andrew, 1955: 178). The US Army used divisional and corps medical battalions for this function and also established convalescent centres in Korea and Japan to enable the minor sick and injured to recover locally and to maximise the ‘return-to-duty’ rates for their forces.
The structures of the forward medical units require junior medical personnel who are properly trained for their military role. It is almost inevitable that personnel in these roles will not have had prior military service and so the volume and quality of recruitment and training for new entry medical personnel is an enduring issue (Griffiths, 1990: 228-229). The content and duration of this training provided by the US Army Medical Department was challenged during the Korean War. This continues to be an issue when the peacetime requirement for military medical personnel is substantially less than the wartime requirement. This necessitates a surge in medical personnel from civilian practice from the Reserves, National Guard or direct conscription who have not been indoctrinated into the difference between military and civilian medical practice (Zimble, 1996: 183-188).
7. Medical Evacuation
It could be argued that aeromedical evacuation as an integral component of a military health system truly came of age during the Korean War (Smith, 1952: 323-332). The introduction of helicopters for medical evacuation (MEDEVAC) is one of the totemic innovations of the Korean War. The full story is covered in DUST OFF: Army aeromedical evacuation in Vietnam (Dorland and Nanney, 1982). In Korea, almost all Army MEDEVAC missions were performed by the Bell Aircraft Corporation’s H -13 Sioux helicopter which had stretcher pods attached to each of the landing skids on the outside of the aircraft. The Navy operated the Sikorski HO33 helicopter in a similar role to support the US marines. Casualties could be transported much faster with a smoother journey than by wheeled ambulances, but they were not provided with any in-transit medical care. There were also problems with the tasking arrangements because there were so few helicopters assigned to the role that control of the assignment of missions was held at Army and Corps level, not Division or Brigade. By the end of the war, over 17,700 patients had been evacuated by Army helicopter. It was claimed that the helicopter had dramatically reduced the time between injury and surgery for battle casualties and saved lives (Neel, 1955: 691-702). However, their true impact on casualty outcomes has recently been challenged, particularly as the primary delay in casualty evacuation occurred in their retrieval from the front line to Battalion Aid Stations which helicopters were unable to undertake (Barr and Montgomery, 2019: S10-S13). The greatest value of the Korean War experience was to create the foundations for helicopter MEDEVAC in the Vietnam War and all subsequent conflicts. As helicopters became more powerful, casualties were able to be carried inside the fuselage alongside increasingly skilled medical attendants. It is likely that the apogee for helicopter MEDEVAC was in Afghanistan in 2010-2012 where several nations were mutually supporting each other with a breadth of helicopter MEDEVAC capabilities that could be tailored to specific missions including collection from contested pick-up points (Bricknell and Johnson, 2011: S444-S448; Olson Jr, et al., 2013: S130-S136).
Perhaps less publicly acknowledged is the rapid development of the US Air Force (USAF) aeromedical evacuation system during the Korean War. After the creation of the USAF as an independent service in 1947, the mission for medical evacuation by aeroplane transferred from the US Army. By the conclusion of the Korean War, the USAF has established itself as a global aeromedical evacuation system using transport aircraft with in-transit care for its patients using USAF medical personnel. The modern aeromedical evacuation system is capable of providing full intensive care support as a ‘hospital in the air’ during transit if needed (Flarity, et al., 2019: 5-20). Likewise the hospital ships of the US Navy, the Royal Navy (HMHS Maine) and the Danish ship, Jutlandia, ferried large volumes of patients from Korea to Japan. They also acted as floating static hospitals to augment the facilities on land in support of battles close to the coast, especially around Seoul. The Korean War demonstrated the importance of inter-Service (army, navy, and air force) and multinational co-operation in the regulation and movement of casualties within a military medical system. This is likely to be a feature of all subsequent conflicts, though the exact balance between ground ambulance, railways, helicopters, aircraft or ships will depend on the nature, location and intensity of military operations (Bricknell, et al., 2019: 173-175; Bricknell, et al., 2019: 176-179).
8. Deployed Hospital Care (DHC)
DHC covers the role and capabilities of field hospitals deployed to military operations away from the home nation of the fighting troops. Alongside helicopter MEDEVAC, the creation of the Mobile Army Surgical Hospital (MASH) is regarded as one of the major innovations of the Korean War (Baker, 2012: 423-429). It followed from the hospital platoons of the US Army field hospitals of the Second World War (King and Jatoi, 2005: 648-656) and was just being introduced as the Korean War broke out (Woodard, 2003: 503-513). The MASH was designed to provide the most forward surgical unit operating in direct support of the combat division. It needed to be mobile so that it could be moved within 6 hours but with sufficient clinical capability that the most challenging operations could be undertaken. The MASH remained within the organisation of the US Army until 2006 when it was replaced by the Combat Support Hospital. As described in the book, The Evolution of Forward Surgery in the US Army: From the Revolutionary War to the Combat Operations of the 21st Century (Steahly and Cannon, 2018), the requirement for flexible surgical units to support military operations remains with continual evolution of the organisational structures to provide this capability.
9. Role 4/Firm Base
The Role 4/Firm Base ‘instrument’ covers the arrangements for receiving military casualties from the theatre of operations and providing restorative treatment, rehabilitation, and long-term support for veterans. Patients were assigned to Army, Navy, and Air Force hospitals by the newly formed Armed Forces Medical Regulating Office. Cowdrey describes the challenges faced by the US military hospitals and the Veterans Administration in the continental USA due to the surge of military patients arriving from the war in Korea. In the years after 1945, the US Army had been forced to close many of its hospitals as a result of budget cuts. Slowly, some closed hospitals were reopened and a full system of rehabilitation for the war injured was re-established.
In the same way that there is unlikely to be sufficient medical personnel in the Active Duty force to fill the posts within an expanded field medical service for any war, it is inevitable the capacity and capability of Role 4 hospital system is unlikely to be sufficient to cope with battle casualties at the beginning of a major conflict. A similar tension occurred in the first decades of the 21st century in many countries with war injured from Iraq and Afghanistan. This resulted in changes to the mental and physical health services provided by the US government through the Veterans Administration and the UK through the National Health Service6) and other agencies (Malish, 2018: 15-26; Voumik, 2015: 56-65).
10. Medical Logistics
Medical logistics is often a neglected component of a military medical system, but it is essential that the medical services are allocated the equipment and material needed to treat casualties. This function was primarily provided by the USA through the despatch of stores being drawn down from across Asia after WW2 and held in Japan. As these supplies began to run out, authority was given to purchase medical material from Japanese production which provided a stimulus to their medical industrial base. The Korean War also provided a reminder of the importance of stretchers and the vital need to recycle them back to the front after casualties have been transferred to hospital beds.
Blood is a uniquely important and challenging commodity for procurement, storage, and distribution within the medical logistics chain. Blood transfusion had become ubiquitous by the end of the Second World War and the US Army blood distribution programme was expanded during the Korean War to cope with the demands of the new conflict. The importance of the blood transfusion service is emphasised by the existence of four separate papers on the topic within the 1954 US Army course on Recent Advances in Medicine and Surgery. Considerable progress had been made to formalise the lessons from World War II and establish a military Blood Committee in the Defence Department and a Blood and Blood Derivatives Group under the Armed Services Medical Procurement Agency. Over the course of the war the number of units of blood administered per casualty steadily rose, reflecting confidence in the supply system and increasing awareness of the value of massive transfusions in severe traumatic shock. As the value of blood replacement in resuscitation became evident, studies were undertaken to identify an alternate to blood that could be used forward of the MASH. Initially, reconstituted serum albumin was used until it was established that Dextran was safe and much easier to manage as it was packaged within plastic bags rather than glass bottles. The wars in Iraq and Afghanistan re-established the centrality of whole blood as the primary fluid for resuscitation and blood products are now routinely available for pre-hospital resuscitation (Gonzales, et al., 2016: S85-S93; Parker, et al., 2015: 2-4).
11. Medical Contribution to Security and Stabilisation
Wars are fought between opposing armed forces with the purpose to achieve a political aim by coercion through the application of violence. This requires the consent of the population to fight the war, particularly in light of the casualties and damage from war. This consent is based upon a political settlement between the government and the people; primarily in the provision of essential services such as security, healthcare, shelter, employment, and education. Any international support to these wider effects can be considered as ‘security and stabilisation’, in which there may be a role for military medical services to support capacity-building with the indigenous military and civilian health services (McInnes and Rushton, 2014: 835-857).
Alongside the deployment of UN forces to fight the North Korean and Chinese forces, it was necessary to rapidly develop and expand the ROK armed forces. This required an expansion of the ROK military medical services. Kang and Park have recently published a review of the challenges and successes faced during this endeavour (Kang and Park, 2023: 463-501). Whilst the ROK military medical system was autonomous, it was provided with assistance and guidance through the United States Military Advisory Group to the Republic of Korea (KMAG) (Duke, 1953: 186-187). US KMAG medical advisers supported the development and equipping of ROK medical units using the US military medical system and structures. Initially civilian medical personnel, either volunteers or conscripts, were assigned to military medical units with very little training. Over time the underpinning infrastructure was established with medical personnel receiving specific training in military medicine at the Korean Medical Field Service School based on the US Army Medical Department (AMEDD) Centre and School at Fort Sam Houston, Texas. In addition to support within Korea, there was also a programme of specialist training in the US for selected ROK military doctors and the establishment of the ROK Army Medical Field Service School, Masan drawing on the methods at the US AMMED Centre and School (Sullivan, 1953: 187-189). These activities provided depth to the US ‘mil-mil’ medical engagement programme. Inevitably there were challenges in the orientation of civilian medical personnel to their military duties, the need to emphasise the return to duty for as many wounded as possible, and some allegations of thefts and false accounting for medical materiel (Cowdrey, 1987: 331). However, by 1953 the US Office of the Surgeon General assessed that the ROK military medical system was probably the best in Asia (Cowdrey, 1987: 332).
Whilst the Republic of Korea had an independent government, at the beginning of the war it lacked the organisational capacity to respond to the grave public health challenges facing its citizens, particularly its internally displaced population. As outlined in the section on Force Health Protection, this was a threat to the manpower of the UN military force as well a humanitarian issue. The head of SCAP’s Public Health and Welfare Section, Brigadier Crawford Sams, deployed to Busan on 1 Aug 1950 to establish a mass program of vaccination, delousing, and hygiene support to refugee camps. Following the recapture of ROK territory, military civil assistance teams worked alongside the United Nations Korean Reconstruction Agency (UNKRA) to establish civil-military assistance offices in every province. Military medical units assisted civilian hospitals and provided part-time instructors in civilian medical colleges. This humanitarian activity was also a key contribution of the other international medical units of the UN force. After the ceasefire, the German government opened a Red Cross hospital in Busan in May 1954 and established a long-term partnership with the ROK health system, both of which should be considered as part of the international contribution to medical support during the Korean War (Kim, 2020). It be argued that the level of immediate and enduring international support for the Korean health system would not have occurred without the Korean War.
The parallel task of using military medical capabilities to contribute to security and stabilisation though humanitarian assistance and health systems strengthening in both the indigenous civilian and military health systems is an enduring feature of many military campaigns. There was similar substantial programme during the Vietnam War as part of the ‘hearts and minds’ campaign (Wilensky, 2004). Similar programmes were established in Iraq (Michaud III and Maxwell, 2012: 676-680) and Afghanistan (Bricknell and Cameron, 2011: S472-S476; Bricknell and Grigson, 2011: S468-S472). This is role now a recognised task for some military health services and is codified under the term military global health engagement covering both ‘military to military’ and ‘civilianmilitary’ activities (Moten, et al., 2018: 14-17).
12. Research and Innovation
As stated in the opening sentence of this paper, war provides a stimulus for medical research and innovation to improve the survival and quality of life for casualties of conflict. The ’hospital’ is the primary location for research into combat casualty care, and the Korean War was no exception. Building upon the multiple research programmes into military medicine during the Second World War, a Surgical Research Team was established by the US at the end of 1951 to conduct clinical investigations into the care of the wounded. The most significant development in military surgical technique from the Korean War was the introduction of vein grafts to repair arterial injuries (Baker, 2016: 258-262). This resulted in a substantial decrease in limb amputation following arterial damage. However, the research into prolonged shock from severe blood loss that was probably the most important area of research. This can result in acute kidney injury causing kidney failure. Using contemporary biochemical analysers and early renal dialysis equipment, the Surgical Research Team codified the clinical course of the condition and the use of dialysis as a temporary treatment pending recovery of renal function. Whilst renal dialysis was used in deployed military hospitals during the Vietnam War, rapid aeromedical evacuation over the last 50 years has meant that this therapy is not considered as a deployed military capability. It may be necessary to reconsider this issue if the character of the conflict precludes rapid evacuation. These lessons for deployed hospital care from the experiences in the Korean War were also noted in papers from senior military surgeons in the British Army (Wright, 1956: 505-510) and the Canadian Army (Davidson, 1953: 1).
Beyond the helicopter and MASH, there are many other examples of medical innovations during the Korean War such as: sledge stretchers for dragging casualties in the snow, converted railway cars for medical evacuation, plastic containers and administration sets for Dextran infusions. Subsequent wars have continued to be a catalyst for medical innovation in clinical sciences, therapies, techniques, and equipment. Many of these have been described in the previous sections. It remains an obligation of the medical leadership to ensure this research is undertaken at an institutional level as well as by individual enthusiasts (Pruitt Jr and Rasmussen, 2014: S57-S65). Whilst the first two decades of the 21st Century have been a highly productive period for military academics (Vickers, et al., 2018: 142-149), it could be argued that it took longer to establish the research systems, trauma registries, and clinical research projects than their predecessors did in the wars of the 20th Century.
13. Mental Health
Whilst not within the list of ‘instruments of military healthcare’, mental health deserves a mention as a separate topic because the impact of war on the mental health of those exposed to conflict is the most researched topic in military medicine (Lewison, et al., 2021: 1829-1839). At the time of the Korean War, the role of combat psychiatry was to preserve the fighting force by returning battle stress casualties to the front line (Peterson and Chambers, 1952: 249-254). Very early in the war US mental health cases were evacuated to Japan and beyond, but this was rapidly reversed based on the experience from World War II that emphasised retention and recovery as close as possible to battle front. In a paper from 2002, Ritchie reviewed the US approach to psychiatry during the Korean War. She notes the link between combat activity and psychiatric cases. She also notes the practice of far-forward early intervention based on the acronym PIES (proximity, immediacy, expectancy) and the use of the term ‘combat exhaustion’ (Ritchie, 2002: 898-903). The provision of mental health support to returning US prisoners of war after the ceasefire agreement was an additional issue. A contemporary paper by Flood describes the British approach to mental health support (Flood, 1954: 40-47). He notes the potential vulnerability of recalled Reservists in the UK 29 Brigade compared to the UK 28 Brigade that was formed from active duty soldiers. Whilst he was based in the Commonwealth hospital in Japan, he recognised that this was too far back in the evacuation chain and he noted that the Canadian Field Dressing Station (FDS) had a psychiatrist to enable it to function as a ‘battle exhaustion centre’ and a screening centre for mental health cases. A more recent review of UK casualty data suggests that the overall rate of combat-related mental health conditions might have been greater than reported at the time because of successful management cases at unit level and at the FDS, and a potential overlap between cold injury and battle stress. It was also noted that British combat units were rotated as complete teams rather than ‘trickle posted’ to establish and maintain unit cohesion (Jones and Palmer, 2000: 256-260). This compares with the introduction of a 5 day period of rest and recuperation (R&R) in Japan for US forces. The Korean War also generated substantial numbers of Korean military and civilian mental health casualties alongside displacing most existing psychiatric patients from their mental health institutions. The US KMAG also supported the development of psychiatric and mental health services to support the ROK forces that influenced the wider revival and modernisation of Korean psychiatry (Lee, 2004: 13-19). This was most immediate in the support of ROK Veterans and it took much longer for mental health services to be developed to care for civilians both for warrelated and non-war-related mental health conditions (Shin and Yim, 2023: 553-591).
The mental health of armed forces personnel was a problem during the Vietnam War and became a substantial issue in the 21st Century for modern all-volunteer forces with soldiers undertaking multiple tours of combat. The need to maximise the number of US soldiers mentally recovered and fit for operations drove a transformation in the organisation of garrison mental health services in US military system in the second decade of the 21st Century (Hoge, et al., 2016: 334-343). The mental health ‘scars’ of war may persist for combatants long after the war has finished. There has been a resurgence of interest in the long-term mental health outcomes for veterans of the Korean War as part of the substantial research programmes that were established to investigate the health outcomes for soldiers deployed to Iraq (including Gulf War 1 in 1990, as well as Gulf War 2 from 2003) and Afghanistan. An overview of posttraumatic stress disorder in US Korean War veterans suggests that they might be a ‘forgotten war’ cohort whose mental health has been relatively under-researched compared to later wars (Palmer, et al., 2019: 554). The Australian government funded a health study of Australian veterans of the Korean War (Ikin, et al., 2007: 475-483). Veterans of the Korean War are an important beneficiary cohort of Veterans Affairs Canada who have health needs that are similar to other veteran cohorts (Thompson, et al., 2016: 70-86). A survey of members of the British Korean War Veterans Association found a correlation between the Combat Exposure Scale and Impact of Event Scale suggesting there were psychological consequences of their experiences (Wild, 2019). Overall, it seems that the principles regarding the prevention and initial management of mental ill-health on military operations learned during the Second World War remained valid during the Korean War, and, indeed, continue to apply (Hourani, et al., 2011: 721-730). Although the long-term mental health consequences of Korean War veterans were not considered at the time, the experience of veterans of the Vietnam War led to the development of the diagnostic label of ‘post-traumatic stress disorder’ (PTSD). Subsequent cohort studies of combat-exposed military veterans (including the Korean War cohort) have shown that PTSD and other mental conditions triggered by military service can have long-term implications for the health and well-being of veterans.
14. Discussion and Interpretation
The overall performance of a military medical system can be assessed by examining the data on national military casualties collated and published by Ministries of Defence. There are three primary summary statistics: Case Fatality Rate (CFR), Died in Action/Wounded in Action Ratio (DIA/WIA), and Died of Wounds rate (DOW). Each is a marker for separate elements of the medical system. The CFR is an indication of the ‘lethality’ of the battlefield, DIA/WIA is a marker of the effectiveness of the pre-hospital system, and the DOW measures the performance of the hospital system. A comprehensive review by Cannon et al of US military casualty data since World War II compared these statistics from World War II, the Korean War, the Vietnam War, and the wars in Iraq and Afghanistan. Overall, the performance of the US military medical system during the Korean War represented an intermediate step in the progressive improvement in the medical care of battle casualties. Notably, there was no statistical evidence of an increase in mortality of battle casualties in the first two years of conflict compared to the other wars, suggesting that the medical lessons from previous wars were applied from the beginning of conflict rather than being relearned by a new generation of military clinicians (Cannon, et al., 2020: S8-S15).
The medical lessons from the Korean War have been characterised by helicopter evacuation and the MASH, possibly because of the TV series of the same name. However, this review of the historical evidence shows that both innovations were evolutionary rather than revolutionary based on extrapolation of developments from World War II. This paper has also shown that the application of modern medical doctrine using the ‘10 Instruments of Military Medicine’ to a historical war provides a framework to identify the many other developments that occurred in military medicine during the Korean War. Each development can be shown to have influenced its field when considered retrospectively over the course of the subsequent 70 years.
However, lessons are learned by people within institutions. This requires lessons to be identified, codified, and then incorporated into doctrine, policy, regulations, and guidance to inform the training and education of the next generation of military health professionals. The medical academic literature is a powerful tool for the former and provides a valuable historical record. However, it is not evidence of institutional change as this can only be proven by reference to internal documents. The papers presented during the course on ‘Recent Advances in Medicine and Surgery Based On Professional Medical Experiences in Japan and Korea 1950-1953’ provide evidence of assimilation of knowledge into an educational programme but this is not evidence of incorporation into institutional document. An example of such institutionalisation is the NATO Handbook on Emergency War Surgery. The first edition was published in 1958 and it is now in its 5th Edition (Cubano, 2018). This is the primary reference source for the training of military surgeons across all NATO nations. Notably, the UK has its own parallel Field Surgery Pocketbook. The first edition was produced in 1944, updated in 1962, and the most recent edition was published as the British Military Surgery Pocket Book in 2004.7) The implementation of the clinical lessons for the care of battle casualties from each conflict can be traced through comparing individual editions of these documents.
The official histories can be exceptional sources of contemporary evidence of experience and lessons. This paper has made extensive use of Cowdrey’s - The Medics War. However, it must be noted that this book was published in 1987, a considerable time after the Korean War and actually after Vietnam War. This delay is similar to the volumes of official histories on medical services published after the Second World War. It is notable that the ‘unofficial-official histories’ of the US and British experience from the conflicts in Iraq and Afghanistan have been published under the auspices of the medical services much sooner to the completion of these campaigns and that there are no ‘official’ histories of these wars.
The written word has value as a processed and analysed formulation of an author’s opinions. In medical practice the process of peer-review tests the validity of this evidence, especially if the opinions are based upon quantitative observations. However, this loses the emotion of personal experience, and also is subject to organisational censorship through the government clearance processes. A lessons or historical analysis also need to consider what might have not gone well. This needs both internal honesty and an analytical framework that considers blind spots. This paper shows how the use of modern concepts for a military healthcare system can be used to seek historical evidence of medical activities for the totality for the endeavour. It also places the narratives and myths into a longitudinal context. It has identified at least two lessons, the use of tourniquets and injections pre-filled with antibiotics, were not institutionalised. Such a historical analysis can be used to teach the relevance of military medical history to a contemporary audience to show how topics and issues are predictable. It may also emphasise the responsibilities of leaders to actively plan to maintain knowledge and collect new observational data from future conflicts (Cannon, et al., 2021: 5-6).
Overall, this paper has drawn upon the history of military medicine from the Korean War and placed it within the context of the evolution of military medicine during the 20th Century and the observations from battlefield experience in the 21st Century. Although the war is now a historical story, many issues that faced military medical personnel 70 years ago remain highly relevant today. This is especially important in the context of the escalation of East-West tensions resulting from the war in Ukraine, the increased bellicosity of China, and the unresolved division of the Korean peninsula.
Whilst there were many advances in military medicine across the ‘10 Instruments of Military Healthcare,’ perhaps the most important lessons concern the military-to-military relations and civil-military relations within the Republic of Korea in the relief of suffering of the non-combatants affected by war. These laid the foundations for the civilian health system that is now equal to that of any advanced economy in the world. As in many other domains of human experience we are left with the challenge of ‘how to convert current affairs into lessons before it becomes history?’ and ‘what is the evidence of success?’ – though examination of evidence in bibliometrics, doctrine and training documentation.